
GI Bleeding Surgery
GI Bleeding is a crisis. Patients present with enormous spewing of blood or hematemsis. The absolute most basic reasons for GI drain are cirrhosis of liver and ulcer sickness. Draining stops all alone's in 90% of the patients. The rest will either require endoscopic treatment or here and there surgery to adequately stop the dying. GI draining can be life undermining if not treated on time. It is transcendently described by drain in the GI tract beginning starting from the pharynx to the rectum.
GI drain can be comprehensively named upper GI and lower GI drain. Upper GI drain begins from the pharynx and ligament of Treitz. Lower GI drain starts from the colon, rectum or rear-end.
Where the causes are confirmed as peptic ulcer, gastric erosions due to alcohol and NSAIDs, gastric varices,
Mallory-Weiss tear, angiodysplasia and gastric cancer the following surgeries are recommended:
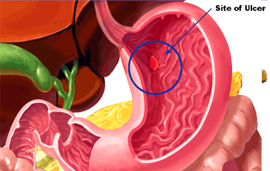
Under-running the ulcer ;Peptic ulcers usually stop bleeding spontaneously. But when
non-operative methods fail, surgery becomes the only option for a life-threatening situation. The simplest way
to stop an ulcer from bleeding is to by underrunning it. The surgery is done under general anesthesia. The
laparoscopic procedure involves making a 11mm port just under the xiphisternum. 2 to 3 stitches are passed deep
into the ulcer and the sutures are tied tight to stop the bleeding. A major part of the procedure involves just
looking for the peptic ulcer which is an extremely tedious and meticulous process.
Pyloroplasty :A pyloroplasty is done to open the lower part of the stomach, a thick, muscular
area called the pylorus. Under general anesthesia, a laparoscopic surgery requires three small incisions in the
area that connect the stomach and the duodenum. Some of the thickened muscle of the pylorus is divided laterally
and cut through to widen it making the connection larger. There are at least three types of pyloroplasty:
- Jaboulay pyloroplasty Without pylorus incision – side to side gastroduodenostomy
- Heineke Mikulicz pyloroplasty longitudinal incision transversely across the pylorus – common procedure
- Finney pyloroplasty With pylorus incision – side to side gastroduodenostomy
Partial gastrectomy :This procedure involves removal of part of the stomach. The procedures
are performed under general anesthesia. A midline incision from the xiphoid process to the umbilicus and
self-retaining subcostal retractors the upper abdomen is explored for metastasis. The part of the stomach is
resected and gastroduodenal anastomosis is achieved after duodenal and omental mobilizations.
Total gastrectomy :This procedure aims at cutting into the abdomen to resect all of the
stomach. A midline incision or a bilateral subcostal incision inferior to the umbilicus is made exposing the
stomach and distal esophagus. Self-retaining retractors provide a wider exposure. The stomach is retracted and
the esophagus is directly connected to the small intestine.
Vagotomy :The vagus nerve which is also called the pneumogastric nerve is resected. There are
many types of vagotomy such as:
- Truncal vagotomy First the pylorus is drained and then divides the main trunk of the vagus.
- Selective vagotomy In this procedure too, the pylorus is first drained and then the anterior and posterior nerves of Latarjet are divided.
- Highly selective vagotomy This is also called proximal gastric vagotomy and involves denervation of the fundus and body of the stomach.
Endoscopic variceal ligation (EVL) :For patients who present with bleeding from esophageal
varices (swollen veins in the food pipe), endoscopic variceal ligation is the treatment of choice and surgery is
usually done as a last resort if all other measures fail. The procedure is done endoscopically where an
enlarged vein or varix in the esophagus ligated with a rubber band. In view of the poor liver condition these
patients are not good candidates for surgery.
Non-cirrhotics are the ones with portal vein thrombosis or non-cirrhotic portal fibrosis also form a large
component of GI bleeding. These patients do very well after surgery because of their preserved liver condition.
Splenorenal shunt and splenectomy with devascularisation :Some patients presenting with
intermittent vomiting of blood or passing melena will require surgical treatment as a permanent cure for
bleeding. Surgery is either in the form of a spleno-renal shunt in non-cirrhotic patients or splenectomy with
devascularisation in cirrhotic patients.
- Splenorenal shunt :In a splenorenal shunt procedure, the vein from the spleen is detached from the portal vein and attached to the renal vein, thereby reducing the varices.
- Splenectomy and devascularization :New procedures for splenectomy and devascularization require that a splenectomy is done first. The distal esophagus is then devascularized through the diaphragm hiatus.
Dr.Patta Radhakrishna is one of the best bariatric surgeons in Chennai. His special area of interest is surgery for Gastro-intestinal bleeding in which he has immense experience. Dr.Radhakrishna has presented his experience in the area of surgery for portal hypertension in many national and international conferences including the Asia-Pacific Hepato-biliary conference in Bangkok and Digestive Diseases Week at New Orleans, USA in 2010.